")
March 20th 2015
After following van der Kolk’s work on trauma and C/PTSD for twenty two years, knowing that his research into the biological nature of PTSD had changed the direction of my life, I finally had a chance to meet him this week. I was sure he would be different from Dan Siegel, but I hoped that he would be approachable and have something interesting to offer.
In fact ‘Bessel’, as most of the audience called him, dressed informally, chatted with us from his podium, comfortably revealed his traumatic childhood, difficulties raising his own children and the forms of therapy that have helped him deal with all of this. Not as revelations, but just as part of a professional conversation with a room full of other therapists. He also commented, and no doubt correctly, that most of this audience would have trauma in their backgrounds – because otherwise they wouldn’t have ended up as trauma therapists! At this there was a murmur through the audience – whether of assent or discomfort I don’t know. And his parting words at the end of two days? That people considering going into therapy should be advised to ask the potential therapist if they have undergone their own therapy – using the system they are about to inflict on this prospective client – and did that system help them? If the answer is “No, they haven’t done their own therapy, or No, they haven’t undergone this particular therapy intervention”, he recommends – leave the room and don’t go back!
Component Elements of the Two-day Workshop/Lecture
1. Neuroscience research into PTSD
2. Neuroscience research into Developmental Trauma – traumatic response to childhood experiences of extreme stress and abuse.
3. Report on van der Kolk’s team’s attempts to have Developmental Trauma Disorder recognized in the DSM-V.
4. Reporting and sharing the therapeutic interventions that have been found to be most effective for adult-acquired PTSD and childhood-acquired Complex PTSD.
5. Bottom line recommendation – that traumatised people need to express their experience through physical and sensory means.
1. Neuroscience research into PTSD
- Looking at Charles Darwin’s writing on the human response to extreme danger, to
 emotional arousal and the link between the danger response and its physical/emotional expression. It is interesting to see that as long as 145 years ago, a scientist was considering the fundamentally physiological nature of the trauma response. Yet this embryonic understanding was lost in the wake of the rise of psychiatry and psychology, until the advent of neuroscience.
emotional arousal and the link between the danger response and its physical/emotional expression. It is interesting to see that as long as 145 years ago, a scientist was considering the fundamentally physiological nature of the trauma response. Yet this embryonic understanding was lost in the wake of the rise of psychiatry and psychology, until the advent of neuroscience.

- The main research reported by van der Kolk involved statistical analyses of the results of standard treatment options for PTSD, compared to yoga/mindfulness meditation, Neurofeedback and EMDR mainly. Results showed better results using yoga/mindfulness and neurofeedback and EMDR compared to antidepressants, anxiolytics, cognitive behavioural therapies and placebos.
Examples:
EMDR vs fluoxetine antidepressant vs placebo
Autonomic arousal level following onset of eye movements
Comparison EMDR vs Prozac and CBT
-

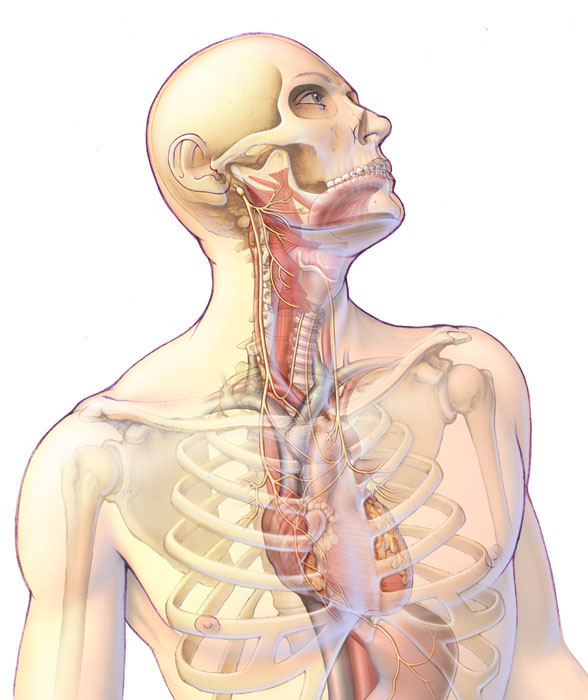
Anatomical overview of the pathway of the vagus nerve
The Vagus nerve. Charles Darwin called this nervous system pathway (cranial nerve X) the ‘pneumogastric’ nerve. He wrote (The Expression of Emotions in Man and Animals, 1872) “Heart, guts and brain communicate intimately via the “pneumogastric” nerve, the critical nerve involved in the expression and management of emotions in both humans and animals. When the mind is strongly excited, it instantly affects the state of the viscera.”

- The need for limbic system therapy – recognition of the dysregulation of arousal
- Recognition of the fundamentally physiological nature of emotions – that they are somatic states that we experience at a bodily level, not ‘psychological states existing in a mental vacuum’.
- Recognition that traumatized people need to have physical and sensory experiences to process their healing
- Left and Right hemisphere anatomy [see Bilateral integration, Integration, under Neurobiology]
- What happens in the brain when the trauma memory is activated?
- Heart Rate Variability (HRV) and Yoga/Mindfulness [see section 4 below]
- The importance of effective action and accessing the emotional brain in overcoming trauma
- Function of the Insula in conveying bodily states to the brain
AFTERMATH OF TRAUMA
Core self:
Feelings as all-or-nothing
- Extreme primary emotions: fear and rage
- extreme secondary emotions & feelings: shame, guilt.
- “Never knowing just what might happen or how it will feel”
Emotions without feelings
- Numbing and alexithymia
- bodily reactions and behaviours without feeling, knowledge or agency
- “Little or no feeling of what happens”
Tortured embodiment and core self
- constantly confronted with the inescapable ‘enemy within’
- feelings are not information to be used; lack of agency
- “The feeling of what happens is often horrible and overwhelming”
Behaviours of the Proto-self (i.e. the false self that develops after trauma)
Dysregulation of arousal
- Exaggerated startle
- Over- or under-aroused physiological and emotional responses
- Difficulty falling or staying asleep
Dysregulation of eating and elimination
- Inattention of needs for food and liquid
- Bingeing, purging and other extreme attempts to sooth body
2. Neuroscience research into Complex adaptation to trauma: Disorders of extreme stress, Developmental Trauma Disorder (the traumatic response to childhood experiences of extreme stress and abuse) and Complex PTSD
Research Statistics
- Questionnaires: Traumatic Antecedents History. ACE Study – Adverse Childhood Experiences Study (http://www.acestudy.org)
- Statistical results of various research studies: Immune function in women with incest histories. Relationship between childhood trauma and borderline personality disorder. Childhood antecedents of self-destructive behaviour. Effects of child maltreatment on Health. ACE studies and scores, showing pervasive problems and outcomes.
Interpersonal Neurobiology
- Attachment studies
- The interpersonal space – states of mind communicating in rhythms and synchrony. Such sharing is the foundation of mental health, therapy, and all learning and education.
- How brains express interest with affection
- The parts that grow most in childhood are those that are needed for learning skills, including language. But these parts are already adapted to their tasks in babyhood, and are ready to engage with other persons’ expressive behaviours.
- Rhythms and Sympathy: the brain coordinates rhythmic body movements and guides them intentionally to interact with the external world, sharing motives and emotions in sympathy with other brains.
- Infants detect regularities in events: rhythmical, predictable interactions help infants form the basis of prediction and causality. Temporal relations between their own sensations and behaviours and the environment. What is likely to happen next. Generates the capacity to plan appropriate action. (Beatrice Beebe, 2010)
- What cannot be communicated to the (m)other cannot be communicated to the self. (Bowlby, 1991)
- Feeling listened to and understood changes our physiology: being able to articulate a complex feeling, and having our feelings recognized, lights up our limbic brain and creates an ‘aha moment’. In contrast, being met by silence and/or incomprehension, silences the spirit. If you hide from yourself that someone molested you when you were a kid, you are vulnerable to react to triggers like an animal in a thunderstorm: with a full-body response to the hormones that signal “danger”.
- Without language and context, your awareness may be limited to: “I’m scared”. Alternating between being inhibited and uptight or reactive and explosive – all without knowing why. (cf. Siegel’s ‘Chaos or Rigidity’)
- Limited life in imagination and symbols.
Second-generational Trauma, e.g. Holocaust offspring
- Epigenetic transmission: Pre-conception – oocytes. Post-conception and pre-natal, in utero. Post-natal, early environment.
Developmental Trauma
ACE Study results (Adverse Childhood Experience): More than 50% with ACE scores of 4 or higher had learning or behavioural problems in school, compared with 3% of those with a score of zero. CHILDREN DO NOT “OUTGROW” THE EFFECTS OF THEIR EARLY EXPERIENCES.
High ACE scores correlated with higher workplace absenteeism, financial problems, pain medications, antidepressants, anti psychotics, and lower lifetime income.
High ACE scores correlate with the following attributable risks for women: depression 54%, suicide attempts 58%, alcoholism 65%, IV drug abuse 78%, victim of sexual assault 62%, domestic violence 52%.
PSYCHOBIOLOGICAL EFFECTS OF SEXUAL ABUSE: 20 YEARS LATER
STUDY BY FRANK W. PUTNAM, M.D., Professor of Paediatrics and Psychiatry, Cincinnati Children’s Hospital Medical Center.
Van der Kolk reported details of this study’s results, looking at groups of survivors of childhood abuse, where the abuse took place at 6 to 12 yrs of age, 12 to 15 yrs of age, and 16 to 23 yrs of age. Putnam’s overall summary of his longitudinal study showed three main areas of damage:
- Serious disorders and high comorbidy (affective disorders, self-mutilation, somatisation, dissociation, problems of conduct, attention, impulse, and hyperactivity)
- Biological Dysregulation (HPA Axis, sympathetic nervous system, obesity, pubertal development)
- Dysfunctional relationships & sexuality (earlier voluntary intercourse, earlier childbearing, more partners, dysfunctional relationships, more domestic violence, more abused children)
Putnam’s study also contains data looking at the dysfunctional categories of Complex PTSD/Developmental Trauma Disorder divided into the sub-groups: Early onset abuse (earlier than 14 yrs old), late onset abuse (14 yrs on), and disaster survivors. This data showed that in all categories of damage early onset abuse rated highest, then late onset abuse, and the percentages for disaster survivors was significantly lower. The categories included the following:
Affect regulation, Anger, Self-destructiveness, Suicidal Intention, Sexual involvement, Risk taking, Amnesia, Dissociation, Guilt, Shame, Nobody can understand, Distorted beliefs, Idealisation of the perpetrator, Loss of trust, Revictimization, Victimising others, Digestive problems, Chronic pain, Cardiopulmonary, Conversion, Sexual problems, Hopelessness and Loss of beliefs.
The differences between the 3 sub-groups are highest in the following:
Self-destructiveness: early onset [EO] twice as high as late onset [LO]
Suicidal: early onset twice as high as late onset. Disaster, low percentage.
Amnesia: early onset twice as high as late onset and 5 times that of Disaster.
Guilt and Shame: early onset nearly twice as high as late onset.
Distorted beliefs: three times as high for early onset compared to late onset, zero in Disaster victims.
Idealization of perpetrator: four times higher in early onset than late onset, zero for Disaster.
Victimizing others: nearly four times higher for early onset than late onset, zero for Disaster. Note however that the overall percentage of the ‘victimizing others’ category is much lower than the other categories listed here.
DIGESTIVE PROBLEMS (!) : 69% for early onset, 60% for late onset, 30% for Disaster. Note: the link between trauma and digestive problems is gaining attention, and biologically may have its locus in the vagus nerve, which links brain, heart and gut.
3. Report on the team’s attempts to have Developmental Trauma Disorder recognised in the DSM-V
High on the list of van der Kolk’s concerns is the intractable stand taken by the psychiatric body that regulates the DSM-V, as he and his colleagues try to change the perception that severe childhood abuse leads simply to a more complex form of PTSD and that treatment for its damage can be conceptualized simply within a PTSD framework. He and his colleagues have conducted many clinical trials to provide evidence that damage to the attachment system is just as important an element in the story, and that the label ‘Complex-PTSD’ might be better replaced by ‘Developmental Trauma Disorder’. The information around this DSM-V disagreement is reproduced under the tab ‘Complex-PTSD or PTSD?’
4. Reporting and sharing the currently most effective interventions for both PTSD and Complex-PTSD (Developmental Trauma Disorder)
A. Adult-acquired PTSD
Van der Kolk presented video evidence and improvement statistics for the following therapeutic interventions, which have shown themselves to have the highest rates of success in lowering PTSD symptoms:


EMDR (Eye Movement Desensitisation Reprocessing)

INTERNAL FAMILY SYSTEMS THERAPY
PSYCHODRAMA or similar styles of Drama Therapy

[I believe TRE (Trauma Release Exercises) should be added to this list. So I will add it, and explain exactly why.]

B. Complex-PTSD (Developmental Trauma Disorder)
Van der Kolk recognises that different interventions are needed for people who have been severely traumatized in childhood, although there is some overlap with the treatments for adult-acquired PTSD. The difference relates to the attachment system damage, and in this respect van der Kolk had to concede to Dan Siegel’s Interpersonal Neurobiology. (The brevity with which he ‘glanced’ at IPNB would seem to suggest to me that there may be some professional rivalry going on there! His powerpoint notes do not reference Siegel at all.)
van der Kolk’s Bottom-Line Recommendation for Complex Trauma Treatment

This conclusion based on trial and experience is in keeping with my own experience over the last twenty years of working in this area. It is echoed by Peter Levine in his book Waking the Tiger, in the emotional release work of the Jamillon Trauma Centre, Arthur Janov who pioneered Primal Therapy and many other similar systems that tap into the body’s natural emotional tension discharge response.
Van der Kolk’s presentation did not offer anything new in this area, which was fine – even rather exciting – because it confirmed that the above pioneers were ahead of their time and that I had been correct in following their example. That was a good feeling.
The importance of van der Kolk’s presentation was that he updated us on the fact that some scientific research had confirmed these approaches as necessary ingredients for healing. This is hugely significant, as scientific research is slowly moving trauma treatment away from the psychiatric/psychology paradigm and towards the physiological/neurological and technological arena.
The link between emotions and their physical expression for health was foreshadowed by Charles Darwin (1872) – “The goal of emotion . . .is to effect physical movement and regain a state of physical equilibrium: the . . . liberated nerve-force . . . produces in us the state we call feeling, [which] must expend and liberate itself in intense sensations, active thought, violent movements, or increased activity of the glands.”
Details of body-based interventions are covered in The Healing Journey.
More on Attachment
