")
PTSD
Post-traumatic Stress Disorder has gone mainstream. Its media and entertainment industry usage is mostly related to the theatre of war, to serious injury and criminal behaviour, such as rape. In the mental health treatment rooms it will usually be picked up pretty quickly, though that doesn’t mean that the clinician will have an in-depth knowledge of how to treat it. The professional PTSD treatment program at the Austin Rehabilitation Centre in Melbourne is only open to returned servicemen, police and fire brigade personel, so civilians have few options for institutional treatment. If this information is out of date I will be very happy for someone to add a comment with any recent programs available for PTSD treatment in Melbourne.
The diagnostic category of PTSD should be applied to a person with the 3-cluster symptoms of Intrusion, Hyperarousal and Avoidance as described under the PTSD tab. These symptoms develop due to either a high impact once-off traumatic event, in childhood or adulthood, or a series of events in reasonably close proximity, which were traumatic but did not involve captivity, loss of freedom over a long period or drawn out torture or brainwashing. In the case of PTSD, the symptoms develop due to the initial shock to the system, followed by failure to successfully integrate the memories of the event, the subsequent intrusion of the implicit memories, and the gradual damage to the nervous system and cortisol levels. Over time, the person’s self-esteem and confidence may be eroded, but this is due to the disabling effect of the PTSD symptoms, not the original traumatic event.
COMPLEX-PTSD (including “developmental trauma disorder”)
Complex PTSD, on the other hand, is a diagnostic category that is most often applied to survivors of severe childhood abuse. However, as detailed under the ‘Childhood Trauma’ tab, Complex PTSD can also be applied to adult-acquired traumatic damage when the traumatic experience was drawn out and involved captivity and maltreatment. The reason that this kind of experience produces a more complex form of PTSD is due to the overwhelming damage to the sense of self, the erosion of a stable sense of self and the long-term experiences of loss of control, self-determination, dignity and safety. In simple terms, the sense of self is ‘broken’. It can take a long time for that degree of damage to be repaired.
Complex-PTSD as applied to survivors of childhood abuse is harder to spot, and is  OFTEN missed in mental health offices. The reason for this is that the usual pattern for an adult survivor of severe childhood abuse (including degrees of severity and degrees of abuse) is to develop secondary mental health problems (known as co-morbid disorders). Most people enter the mental health system seeking help for these secondary problems. If the clinician does not know the right questions to ask, the original childhood traumas may go unattended or unrecognised, often for years! This is where the approach of ‘treat the current problems and help the person get their life working functionally’ may appear to work, but will leave the source of the problem and the lack of integration, unresolved and festering.
OFTEN missed in mental health offices. The reason for this is that the usual pattern for an adult survivor of severe childhood abuse (including degrees of severity and degrees of abuse) is to develop secondary mental health problems (known as co-morbid disorders). Most people enter the mental health system seeking help for these secondary problems. If the clinician does not know the right questions to ask, the original childhood traumas may go unattended or unrecognised, often for years! This is where the approach of ‘treat the current problems and help the person get their life working functionally’ may appear to work, but will leave the source of the problem and the lack of integration, unresolved and festering.
WHAT TO LOOK FOR . . .
If a clinician has been employed to help a client learn strategies for improving her present-day problems, but is aware of the possibility of childhood damage, what clues or indications might have alerted her to this possibility? Below is a list of some of the more common indicators. It is when the client starts to disclose a cluster of these signs that the clinician should begin to show interest in looking further back in that person’s life and getting more information about the early years:
The client’s general sense that ‘things aren’t working’
Continual difficulties with relationships (intimate, workplace, family, friends)
Pattern of choosing dysfunctional partners
Anxiety and/or depression
A realization that something is strange/different about the way their mind works
Their inner emotional life has some odd features about it
Suicidal feelings
Had postnatal depression after birth of child
Had or has an eating disorder
Had or has degrees of obsessive-compulsive behaviour
Has experienced strange triggered feelings when reading about certain key topics, such as ritual abuse, child sexual abuse, child psychological or physical abuse, peadophile groups etc.
Has been in and/or coming out of a relationship with a psychopath or malignant narcissist
Has recently suffered a traumatic experience and has developed PTSD symptoms
Forms co-dependant relationships which eventually don’t work
Has chronic gastric and intestinal problems, (gastroparesis, irritable bowel syndrome, reflux etc.)
Emotional difficulties flow over into medical difficulties
Is lonely, isolated and unable to form stable relationships
Has been diagnosed by psychiatrist/psychologist as having a mental health disorder from the DSM V, especially Borderline Personality Disorder
Disabling problems with self esteem and sense of self
Chronic need for approval and subjection of own needs
If the therapist is gentle and cautious in her approach, and does not introduce ideas about the past that the client has not mentioned, there is little danger in opening up discussion of childhood memories. The therapist is opening a door, just opening it. She waits respectfully and allows the client full control as to if, how and when she chooses to walk through. If there is no trauma there, the client will not find it. She may simply find some family dysfunctions that need bringing to the light, as these family patterns may be playing out unconsciously in the client’s life. A large part of therapy is bringing dysfunctional patterns to the client’s attention and awareness. With awareness there are then choices that can be made for change.
C-PTSD or DEVELOPMENTAL TRAUMA DISORDER ?
BESSEL A. VAN DER KOLK on the Diagnostic Category relating to Childhood Trauma/Abuse
(This information is taken from van der Kolk’s seminar in Melbourne, March 2015)
PROPOSAL TO INCLUDE DEVELOPMENTAL TRAUMA DISORDER in the DSM V
Bessel A. van der Kolk & Robert Pynoos MD et al.
Statement of Purpose: [extract]
The goal of introducing the diagnosis of Developmental Trauma Disorder is to capture the reality of the clinical presentations of children and adolescents exposed to chronic interpersonal trauma and thereby guide clinicians to develop and utilize effective interventions and for researchers to study the neurobiology and transmission of chronic interpersonal violence.
The introduction of PTSD in the psychiatric classification system in 1980 has led to extensive scientific studies of that diagnosis. However, over the past 25 years there has been a relatively independent and parallel emergence of
- the field of developmental psychopathology (eg Maughan & Cicchetti, 2002; Putnam, Trickett, Yehuda & McFarlane, 1977), which has documented the effects of interpersonal trauma and disruption of caregiving systems on the development of affect regulation, attention, cognition, perception, and interpersonal relationships.
- The other significant development has been the increasing documentation of the effects of adverse early life experiences on brain development (eg De Bellis et all, 2002; Teicher et all, 2003), neuroendocrinology (eg, Hart, Gunnar & Cicchetti, 1995) and immunology (eg, Putnam et all, 1997; Wilson et al, 1999).
A survey of 1,699 children receiving trauma-focussed treatment . . . . showed that the vast majority (78%) was exposed to multiple and/or prolonged interpersonal trauma. Less than a quarter met diagnostic criteria for PTSD. Fewer than 10% were exposed to serious accidents or medical illness. Most children exhibited posttraumatic sequelae not captured by PTSD: at least 50% had significant disturbances in affect regulation; attention & concentration; negative self-image; impulse control; aggression and risk taking.
Whether or not they have symptoms of PTSD, children who have developed in the context of ongoing danger, maltreatment and inadequate caregiving systems are ill-served by the current diagnostic system, as it frequently leads to no diagnosis, multiple unrelated diagnoses, an emphasis on behavioural control without recognition of interpersonal trauma and lack of safety in the etiology of symptoms, and a lack of attention to ameliorating the developmental disruptions that underlie the symptoms.
The team proposed a body of criteria for Developmental Trauma Disorder, which (here summarized briefly), includes:
1. Exposure (direct experience or witnessing of repeated, severe episodes of interpersonal violence, and significant disruptions of protective caregiving, repeated separation from primary caregiver or exposure to severe and persistent emotional abuse.)
2. Affective and Physiological Dysregulation (Inability to modulate, tolerate or recover from extreme affect states; disturbance in regulation in bodily functions such as sleeping, eating, elimination and over- or under-reactivity to sensory stimulation; diminished awareness/dissociation of sensations, emotions and bodily states; impaired capacity to describe emotions or bodily states.
3. Attentional and Behavioural Dysregulation (preoccupation with threat or impaired capacity to perceive threat; impaired capacity for self-protection; maladaptive attempts at self-soothing; habitual self-harm; inability to initiate or sustain goal-directed behaviour.)
4. Self and Relational Dysregulation (intense preoccupation with safety of the caregiver or loved ones; persistent negative sense of self; persistent distrust defiance or lack of reciprocal behaviour in close relationships with adults or peers; reactive physical or verbal aggression; inappropriate attempts to get intimate contact or excessive reliance on others for safety and reassurance; impaired capacity to regulate empathic arousal, ie, lack of empathy or excessive responses to the distress of others.)
5. Posttraumatic spectrum symptoms
6. Duration of disturbance, more than 6 months
7. Functional Impairment in two or more of the following – scholastic under-performance, familial conflict, peer group relationship, legal/criminal, health.
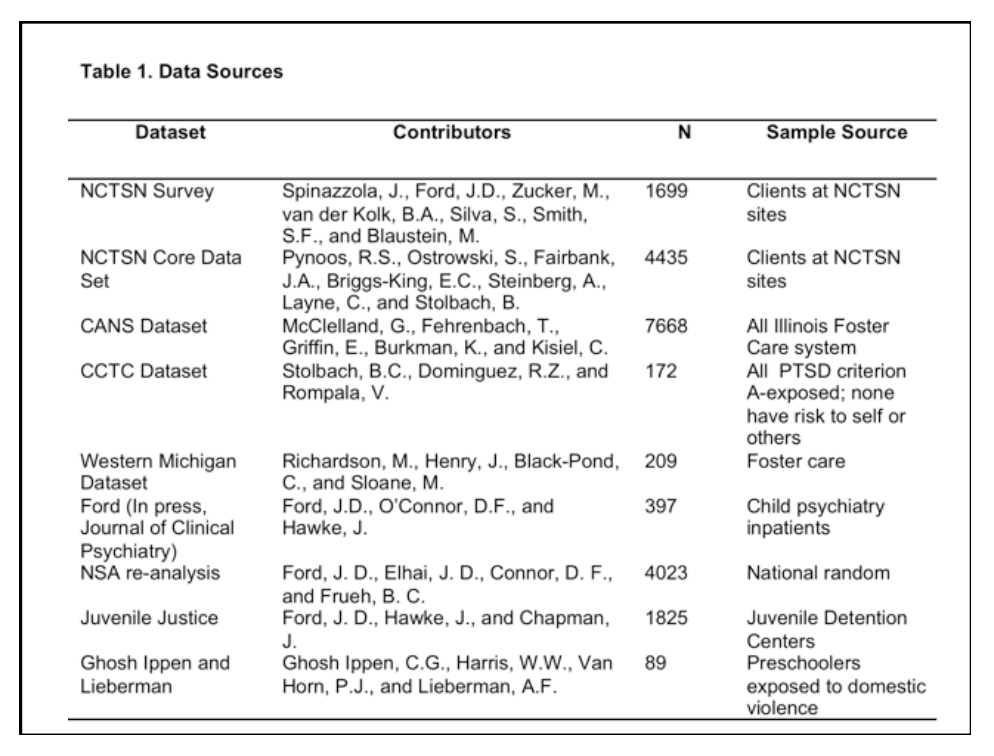
The proposal was accompanied by documentation of the extensive trials and research carried out by many practitioners in the field. The column N indicates the size of population sampling :
The DSM V taskforce response:
The consensus was that there is just too little evidence, at this time, to include DTD in the DSM-V. There have not been any published accounts about children with this disorder. There have been no predictive validity tests. And there have been no studies on differential responses to treatments. In short, a number of reviewers felt that your proposal read more like a concept paper, rather than as a scientific proposal for a new syndrome. The notion that early childhood adverse experiences lead to substantial developmental disruptions is more clinical intuition than a research-based fact. This statement is commonly made but cannot be backed up by prospective studies.
In van der Kolk’s opinion, the DSM-V is an ever expanding smorgasbord of trauma-related “co-morbidities”, based on a deficit model of mental disorders. Most worrisome perhaps is that of the nine symptoms of Borderline Personality Disorder, all are clearly represented in the proposed DTD symptoms (B1, B2, B3, C1, C2, C4, C5, D1, D2, D3, D4, D5, D6) [apologies that the attributes of these numbers have been lost in my summary of the proposal] (From Herman, van der Kolk and Perry, ‘Childhood trauma and borderline personality disorder, American Journal of Psychiatry, 1989)
87% of subjects with BPD had histories of severe childhood abuse and/or neglect starting prior to age 7.
More on C-PTSD / Childhood Trauma
The Hidden Experience of Abuse
Further Resources and Readings (Childhood Trauma)
