")
The study of trauma has probably been the single most fertile area within the disciplines of psychiatry and psychology in helping to develop a deeper understanding of the interrelationships among emotional, cognitive, social and biological forces that shape human development.
Van der Kolk, in Solomon & Siegel (2005), p.189
The introduction (“Trauma”) put forward the conceptualisation that ‘trauma’ is a wound (or series of wounds) that needs healing in some kind of physical reality. So what is that physicality and where is it located? The (potentially) traumatic experience is registered in the person’s brain, via their sensory organs and the pathways that transfer sensory data to the relevant organs in the brain that filter, analyse and respond to incoming data. It is in the overload of emotional data (i.e., our response to what we are witnessing or experiencing) that the breakdown happens.
TRAUMA, in the first instance, is caused by the brain’s failure to synthesize and integrate the sensations (immediate experience) of the event into an integrated (visual, verbal, emotional, sensory) memory. Instead, sensory elements of the experience are stored separately, and retrieved as isolated emotional, sensory, physiological and cognitive fragments, often unconnected to the original event. Healing from trauma must include some integration (or linking) of the aspects of the experience into a coherent narrative with a beginning, middle and end.
An event is not inherently traumatic. What makes it become traumatic is our response to it, our interpretation of what we have witnessed or experienced. (That statement recognises that certain events will in most cases be traumatic for most human beings. But the statement, in a philosophical sense, is correct and will be expanded upon in further sections.)
LINK TO “NEUROPLASTICITY 101 FOR TRAUMA SURVIVORS” ~ a Highway metaphor encapsulating the experience of trauma in the brain. Just a quick detour from the more complex information below.
The Nervous System’s Response at the time of the Overwhelming Event
CONTENTS
1. The Sympathetic Nervous System (puts us on high alert)
2. The Fear Response (part of the Sympathetic system, automatic function)
3. The Restraint System (if the high alert is unnecessary, OR we can problem-solve our way out of the emergency, helps override the Fear Response)
4. The Parasympathetic Nervous System (brings us back down to baseline/normal level of functioning, either because danger is past, or was misinterpreted as danger)
1. Malfunction of the emergency stress response system at the time of the traumatic event
The onset of stress triggers a natural and protective hormonal response in animals and humans, controlled by the endocrine system in response to signals from the amygdala. It is known as the Sympathetic Nervous System. [see diagram]
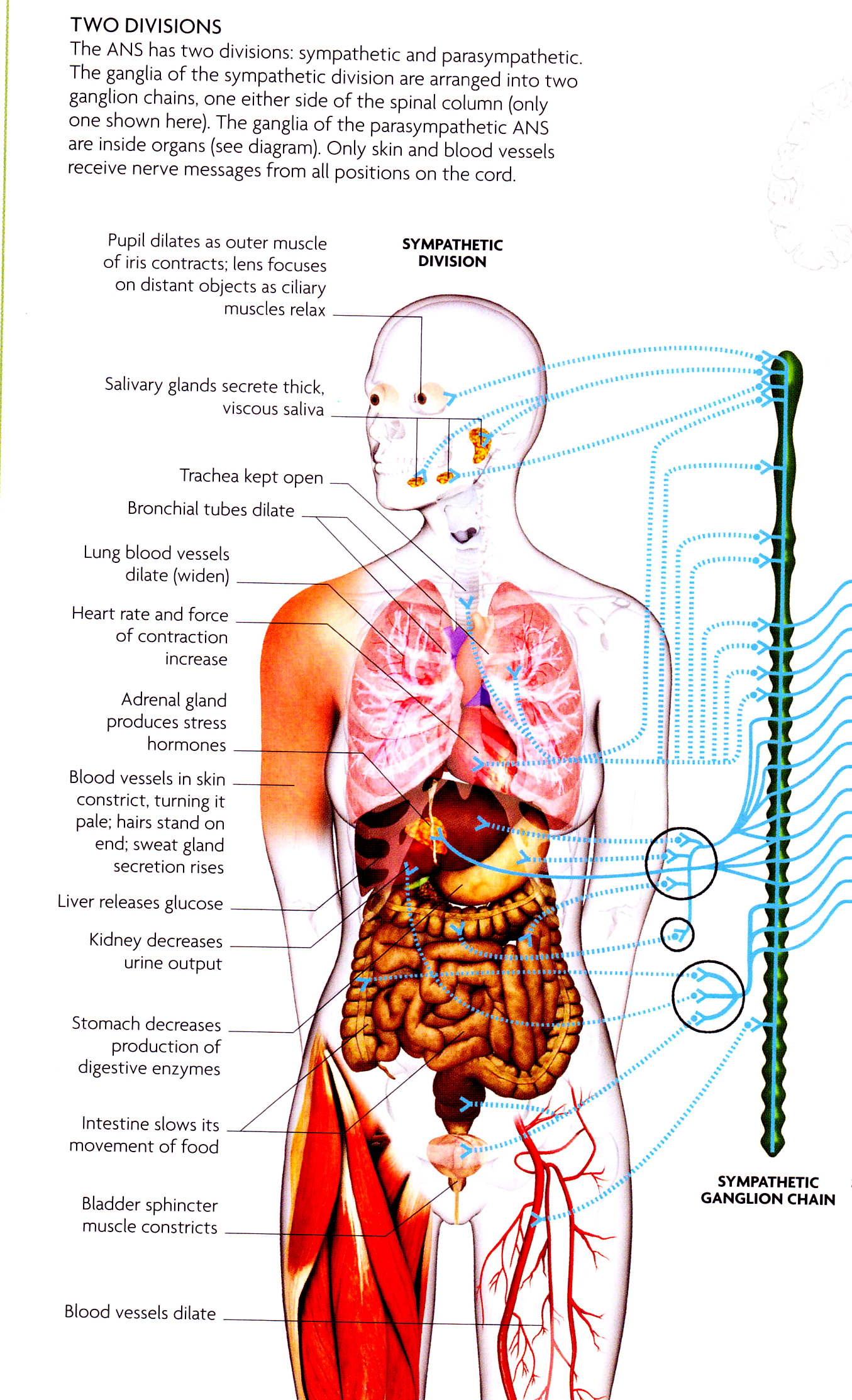
Stress response, often referred to as the “fight-or-flight” reaction, is your body’s rapid and automatic switch into “high gear.” It’s easy to imagine how this reaction helps you deal with a physical threat. You need the energy, speed, concentration and agility either to protect yourself or to run as fast as possible.
When you encounter such a threat, the hypothalamus, a tiny region at the base of your brain, sets off an alarm system in your body. Through a combination of nerve and hormonal signals, the sympathetic nervous system prompts your adrenal glands, situated atop your kidneys, to release a surge of hormones — the most abundant being adrenaline and cortisol.
Adrenaline increases your heart rate, elevates your blood pressure and boosts energy supplies. Cortisol, the primary stress hormone, increases sugars (glucose) in the bloodstream, enhances the brain’s use of glucose and increases the availability of substances that repair tissues.
2. The Fear Response : The complex alarm system also communicates with regions of the brain that control mood, motivation and fear (limbic system).
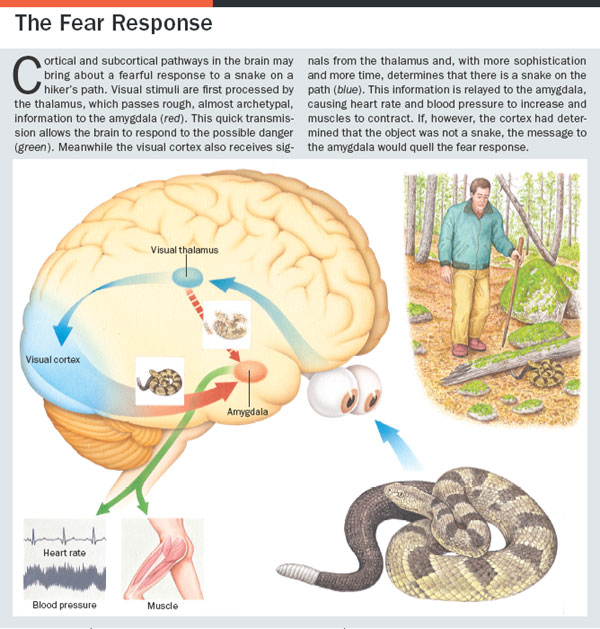
[Siegel, Marc. ‘Can we cure Fear?’ Scientific American Mind 16, pp 44-49 (2005)]
3. The restraint system is suggested in the picture narrative above, but is illustrated more explicitly in ‘Emotional Memory’ below. The reason I include this second diagram is to emphasise the function of the prefrontal cortex in curbing the ‘panic button’ of the amygdala. This is the neural network explanation behind the effectiveness of cognitive behavioural therapy strategies. Our brains are wired to be able to take charge of dysfunctional emotion responses.
The Amygdala and its link to the Prefrontal Cortex

4. When the emergency is past, the Parasympathetic Nervous System [see diagram] decreases hormone levels and enables your body to return to normal. As levels of the hormones in your bloodstream decline, your heart rate and blood pressure return to normal, and other systems resume their regular activities. Note that the same parasympathetic ‘wind down’ happens if the frontal cortex can successfully calm the amygdala’s overreaction due to either a false alarm or a triggering of traumatic memory.
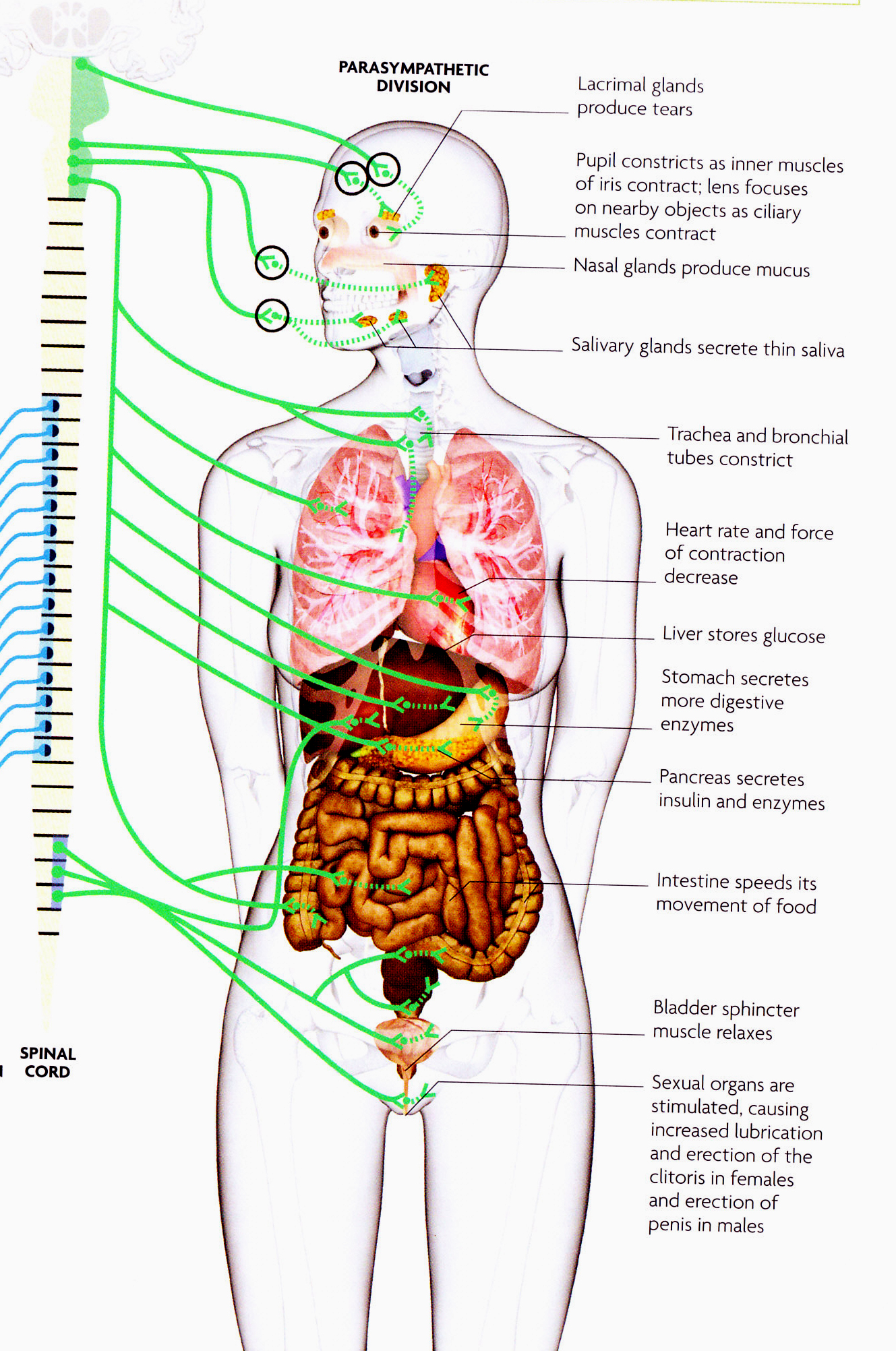
Hormones involved in stress responses and readjustments : to activate flight or fight response : catecholamines (epinephrine, norepinephrine), glucocorticoids, cortisol. To adjust back to normal : the same cortisols – epinephrine, norepinephrine, as well as the ‘feel good’ hormones – vasopressin, oxytocin and endogenous opioids.
In the case of an event of overwhelming terror, shock or stress, especially one from which there is no ability to escape, the mind responds by dissociating. Without some degree of focussed attention, the memories of the event cannot be successfully processed and the normal functioning of the amygdala, the hippocampus and the frontal cortex (higher brain) is suppressed.
Failure of the Information Processing System to process and integrate incoming stimuli
The failure of the central nervous system to integrate an overwhelming experience is due to the effect of extremely heightened emotions on the amygdala. The amygdala helps to assign importance and significance to incoming stimuli and communicate this to the hippocampus, which then acts to encode the experience into the short term memory system, and later, into the long term memory. (Only when the details of the event are encoded into permanent memory are they free of the hippocampus and mediated by the neocortex. See PTSD/Implications for Treatment)
If the amygdala is flooded with cortisols through extreme stress, its messages to the hippocampus are interrupted, as the hippocampus goes offline. Instead of going through the usual routes from short term to long term memory via the hippocampus, the memories are shunted into the implicit memory system, and are no longer available to the cognitive systems in the cortex that would normally assess them, sort them out and discard what is not useful and file the relevant information for future benefit. Another way of putting this is that the ‘implicit’ elements of the experience – sensory perception, bodily responses, emotion and behavioural responses – would normally be stored as context-dependent memory associated with the autobiographical, narrative memories of the same event. Under traumatic conditions, only the context-dependent elements are stored in the automatic memory system, while the consciously retrievable elements (the linear narrative) have failed to be successfully processed and stored.
Implicit memory involves the perceptual, emotional, and behavioral neural responses activated during an experience. It is likely that our bodily sensations are also a form of implicit memory, but these have not been formally studied in research paradigms. Mental models, or generalizations of repeated experiences called “schema,” are also a form of implicit memory.
Once in the implicit (automatic) memory system, the highly emotionally charged memories continue to intrude into consciousness, but not as normal, explicit and autobiographical memory. Implicit memory has no past tense, and is constructed as sensory and emotional data in the neural network. It intrudes as chaotic and persistent flashbacks of the experience, and feels as if it is happening NOW. The person finds themselves continually thinking about, replaying and re-experiencing an event that is distressing, frightening and deeply disturbing.
This is what Trauma is. The two key systems are the central nervous system and the information processing system of the brain’s neural network. If the damage to these systems is not treated, and the feedback loop continues, the likelihood is that the person will develop posttraumatic stress disorder. This is dealt with under PTSD.
Why does one individual fail to make sense of an overwhelming experience and become traumatised, while another heals normally from the same experience?
The answer to this lies in the following variables :
- The age of the person when the event happens (younger=worse)
- The length of the event or number of repetitions (more=worse)
- The social support available after the event (more=better)
- The personal background of the individual and whether there are prior traumas in that background. (most stable, least traumas=better)
- The belief systems and mental models that drive the individual’s response to life’s unpredictable events. (most flexible=better)
- Coping style during the event. (problem-solving style=better)
Examples of the issue of belief systems influencing a person’s interpretation of the event :
A bystander at a bank robbery : (based on an actual event)
Response 1 : religious belief system, it is ‘the will of God’ if I die, so I will just surrender the outcome. (probably won’t develop PTSD)
Response 2 : the men in my family have always protected me. Why aren’t they here now to keep me safe? I feel abandoned, my world has fallen apart. (probably will develop PTSD)
Victim of a car crash : (based on an actual event)
Response 1 : Life is random and people make mistakes. It wasn’t anyone’s fault, just happened. (probably won’t develop PTSD)
Response 2 : Life should always be fair and people should behave responsibly.
OR – The person who hit me should have behaved nicely and apologized, but he didn’t. I am a victim here! It’s NOT FAIR! (might develop PTSD if other factors contribute, i.e., has had prior disempowering experiences which have not been resolved, and continues to dwell and obsess about the event.)
More on “Trauma”:
The Neurobiology of Psychological Trauma
An Evolutionary Model of Response to Danger
The Brain’s “Information Processing System”
Further Resources and Reading (Trauma)
