")
In the field of psychiatry and psychology, the term “dissociation” is used in connection with trauma, overwhelming experiences, extreme anxiety, and their consequences. It is usually used in a context of states of distress, fear, panic, conflict and heightened emotions. In this context dissociation is the individual’s automatic response to situations that feel overwhelming and beyond one’s capacity to deal with. However, in a wider, everyday context, dissociation is a universal human experience, which most people experience at some time.
Normal (non-pathological) Dissociation
The essence of the normative dissociative process is absorption, intense focal concentration and cognitive involvement in one (or more) aspect(s) of conscious awareness, resulting in the exclusion (dissociation) of other content from the phenomenal field.
Day dreaming (allowing the mind to wander where it perhaps needs to go)
Immersion in recreation (a psychological vacation from life’s stresses)
Successful engagement in activity of personal significance (prayer, sex, meditation)
Engagement in peak experiences, during which the person may experience a loss of self-awareness and time, and some perhaps even moments of derealization or depersonalization.
Deliberately induced trance states and religious exctasy.
The ‘adaptive’ function of absorption is to complete certain necessary mental processes, albeit at the expense of tracking intervening events.
Recent Models of DISSOCIATON
as they pertain to TRAUMA, PTSD & DEVELOPMENTAL TRAUMA DISORDER
CONTENTS –
Introduction to Dissociation as a Disorder (from Spitzer et al, 2006)
Proposal of two types of Dissociation: Detachment & Compartmentalization (from Brown,R.J.,2006) Definitions, Manifestations and Mechanisms
Earlier model of Dissociation (from Daniel J.Siegel, 1999, 2nd Ed. 2012): dissociative phenomena driven by two different systems – Parasympathetic Nervous System and Information Processing System.
Dissociation and Memory
INTRODUCTION
from Spitzer et al (2006) “Recent Developments in the Theory of Dissociation”
Published in World Psychiatry, 2006, June; 5(2): 82-86
PATHOLOGICAL DISSOCIATION
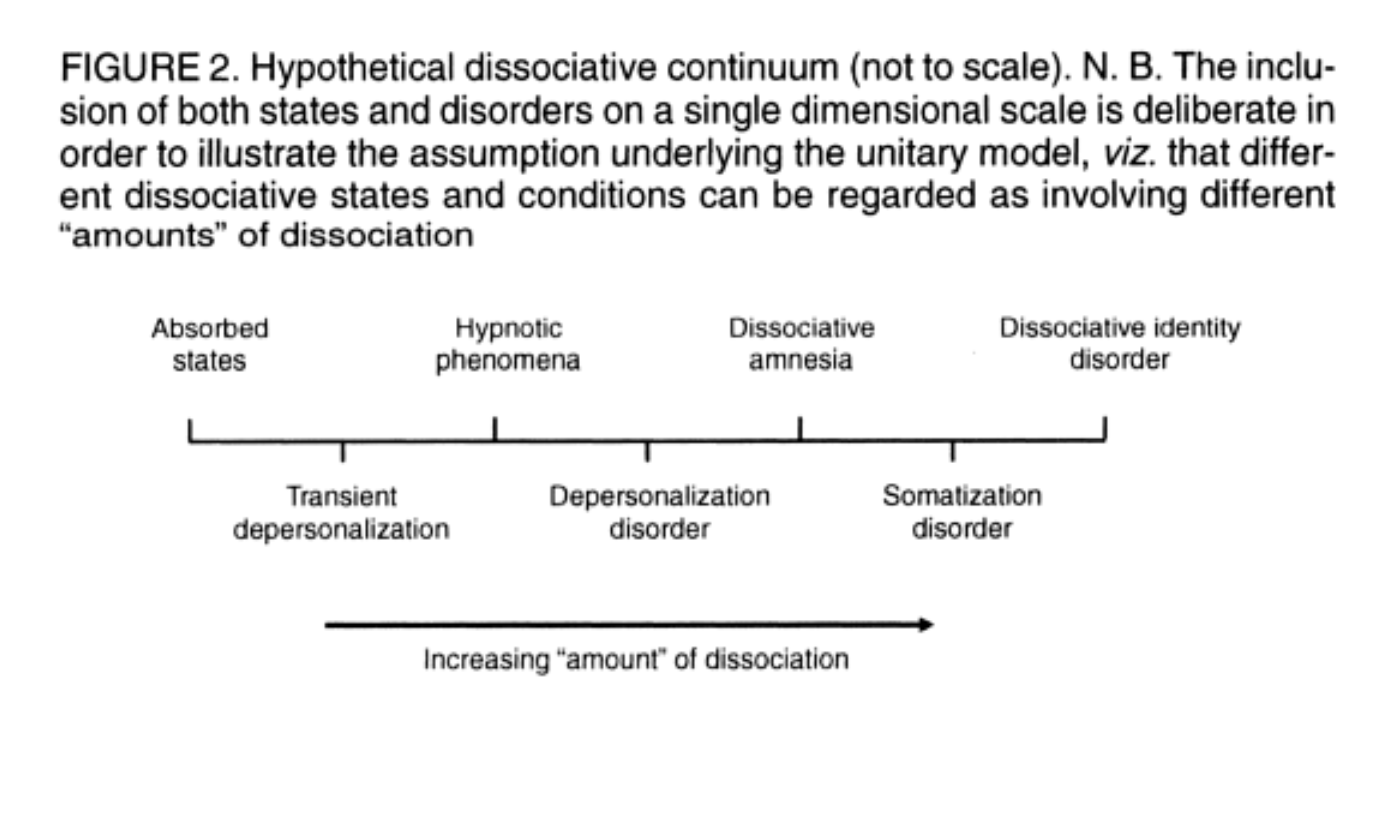
At the end of the 19th century, Pierre Janet elaborated the concept of dissociation, viewing the phenomenon as particular to mental disorders and absent in healthy people (therefore a typological approach [see definition next paragraph, Ed.]). Contemporary and later investigators conceptualized dissociation as a dimensional process, ie, existing along a continuum from normal, relatively common experiences such as daydreaming, to severe and clinically relevant forms seen in dissociative disorders.
Until recently, this so-called “dissociative continuum” has been one of the prevalent key principles in the field of dissociation. However, the controversy about whether dissociation represents a dimensional or typological construct has re-emerged. Analysis of respondents’ answers on the Dissociative Experiences Scale (DES – the most widely used self-report measure of dissociation) has validated the distinction between a dimensional, non-pathological type and a discontinuous, pathological, “typological” class of dissociation.
Since there is no consistent agreement about precisely what dissociation “is”, it was Cardena’s valuable contribution to provide an elaborated and systematic overview of the various uses of the term. He described dissociation in three distinct ways:
as a lack of integration of mental modules or systems,
as an altered state of consciousness,
and as a defense mechanism.
While the third category largely reflects the function of the other two, the first and second category qualitatively differ from each other. The majority of recent conceptualizations converge on this dichotomy, and it has been suggested to label these two types of dissociation as “compartmentalization” and “detachment”.
DETACHMENT & COMPARTMENTALIZATION
From Brown, R.J. (2006) “Different Types of Dissociation have Different Psychological Mechanisms”
Published in Journal of Trauma and Dissociation, 7, 7-28, 2006
All the information on the Detachment/Compartmentalization model of dissociation is taken directly from R.J.Brown’s article, but I have changed the neuropsychological language in places to make the text easier to understand.
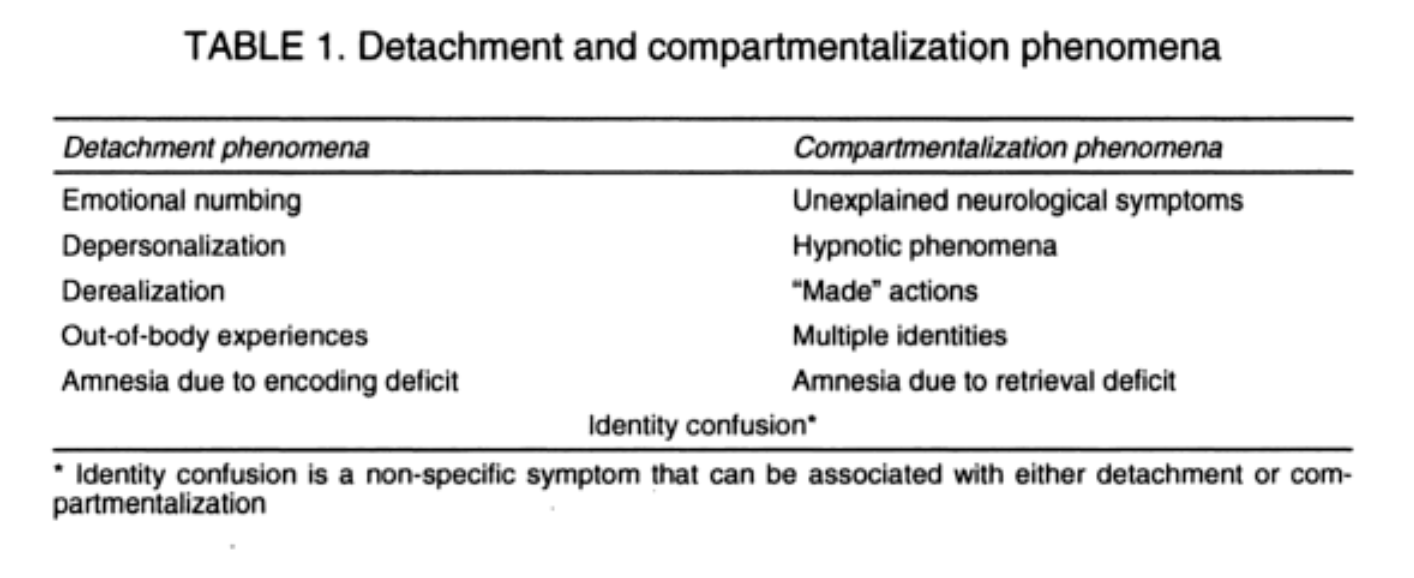
DETACHMENT
Detachment is a form of dissociation in which the medial prefrontal cortex interferes with the normal working of the limbic system in its processing of emotion. It is described as a ‘dimensional’, non-pathological phenomenon existing along a continuum from normal to dysfunctional and chronic.
DEFINITION & DESCRIPTION
An altered state of consciousness characterized by a sense of separation (or ‘detachment’) from aspects of everyday experience (Holmes et al, 2005)
The sense of detachment may relate to the individual’s emotional experience (as in emotional numbing), their sense of self (as in some depersonalization phenomena), their body (as in out-of-body phenomena), or the world around them.
Descriptions of detachment include an absence or alteration of emotional experience, feelings of being “spaced out”, “disconnected”, “unreal” or “in a dream”, a sense of being an outside observer of one’s body, and perceptions of the external world as flat, lifeless and “strange”.
Sometimes detachment dissociation seems to produce memory disturbance and even amnesia, but Brown believes that the mechanism is different to that of compartmentalization. The experience of detachment-type dissociation may manifest as a distinct disorder or as part of a wider disorder such as anxiety disorder or PTSD. It is commonly experienced at the time of a traumatic event, in which case psychiatry labels it ‘peri-traumatic dissociation’ associated with Acute Stress Disorder. (If untreated, ASD will usually develop into PTSD.)
Mild and transitory experiences of detachment dissociation are reported associated with fatigue, intoxication and stress. These fall on the lower end of the dissociation continuum, and as stress, distress and disability rise, so the symptoms of detachment dissociation increase in severity.
MECHANISMS OF DETACHMENT DISSOCIATION
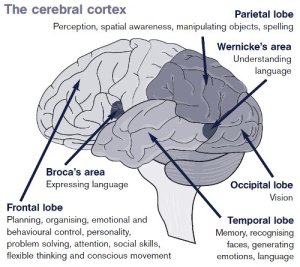
Researchers propose that detached states are produced by hard-wired biological defense mechanisms. These have evolved to help us lessen the potentially disabling effects of extreme stress under threatening situations. A strong-enough rise in anxiety causes the medial prefrontal cortex (see diagram) to inhibit the ability of the limbic system to process emotion. This in turn reduces the output of the sympathetic nervous system which switches the body into high alert. The absence of high emotion allows for more ‘clear-headed’ adaptive behaviour in the face of threat.
In depersonalization disorder, this state of emotional shut-down has become chronic, and Brown reports research that suggests that the detached state may become chronic as the individual misinterprets the state of detachment itself as a threat (ie, a symptom of impending mental breakdown). This fear perpetuates the anxiety and emotional shut-down.
Research indicates that depersonalization and derealization are associated with anxiety, and that this anxiety is targeted at specific stimuli, not just random unpleasant stimuli. The brains of subjects with depersonalization disorder, when shown aversive pictures, show increased neural responses in areas dealing with emotional regulation, and decreased neural responses in the areas activated by emotional stimuli.
The neuroscience at this point indicates a hard-wired neurophysiological profile for detachment-type dissociation. The phenomenon is also seen in certain neurological conditions and drug states.
Judith Lewis Herman, in Trauma and Recovery, describes ‘constriction of consciousness’ that is part of the dissociative consequences of post-traumatic stress:
‘Events continue to register in awareness, but it is as though these events have been disconnected from their ordinary meanings. Perceptions may be numbed or distorted . . . Time sense may be altered, often with a sense of slow motion, and the experience may lose its quality of ordinary reality.’
(Herman, J.L., 1992, pp.42-43)
COMPARTMENTALIZATION
Compartmentalization is a form of dissociation that takes place in the frontal lobes of the neocortex, where executive functions are carried out. This is the ‘typological’ form of dissociation, ie, a discrete, pathological condition (rather than a ‘dimensional’ one existing on a continuum from normal to pathological, as in Detachment).
Definition and Description
- Compartmentalization involves a breakdown in the ability to control processes or actions that would normally be able to be controlled (examples: amnesia – it is normally possible to recall an event 30 minutes after it’s happened; hysterical paralysis, in which part of the body is paralysed, even though there is nothing physically wrong with it.)
- This breakdown in control cannot be overcome by an act of will
- The results are reversible, at lease in principle, under effective conditons with effective interventions,
- it can be shown with relevant diagnostic equipment that the disrupted functions are actually operating normally and are continuing to influence cognitions, emotions and actions.
Dissociative phenomena produced by compartmentalization:
- Amnesia, Dissociative Fugue, Dissociative Identity Disorder, Conversion Disorder, Somatization Disorders.
- Phenomena produced by hypnotic suggestion: amnesia, anaesthesia, pseudohallucinations, motor disturbances etc.
- “Made” actions – actions that the individual does not feel that they are controlling.
Brown suggests that compartmentalization may also exist along a continuum of distress and disability, from non-pathological experience produced by hypnotic suggestion, through temporary amnesia and conversion symptoms, to the chronic disorders of DID and somatization. But in each case the apparently disrupted function is said to be ‘compartmentalized’. This will be discussed further in the next section, mechanisms of compartmentalization.
Laboratory and experimental examples:
- Amnesia following epileptic seizures compared to non-epileptic seizures.
Two groups who both experienced amnesia for the events happening during their seizures: one group had generalized epileptic seizures (true epilepsy), the other group had seizures that were not caused by true epilepsy. Both groups were hypnotized some time after the seizures and given hypnotic suggestions for recovery of memory of the events happening while they were having the seizures. (All information recovered was verified independently.)
The result showed that 85% of the non-epileptic seizure patients recalled information for which they had previously been amnesic, compared to 0% in the true epilepsy group.
What this study showed was that the non-epilepsy seizure patients had encoded information during the seizure but had compartmentalized it within the cognitive (and perhaps implicit – Ed) systems, rendering it unavailable for deliberate retrieval. Presumably the genuine epileptic patients had been unable to encode the information due to a biological brain dysfunction during the seizure.
[compare with detachment dissociation, in which amnesia may also be a failure of encoding, unlike compartmentalization. This has not been verified however.]
- Conversion disorder – ‘implicit perception’
A test subject with blindness in one eye caused by conversion disorder. Visual images of three triangles were presented to his blind side and he was asked to identify which triangles were oriented differently to the others on the screen. Despite being unable to ‘see’ them, he made intuitive guesses, of which 74% were correct, an above-chance response. This indicated that his brain was actually receiving visual information about which he was unaware, due to the compartmentalization process in conversion disorder.
This subject’s performance in the test improved when he was told that he appeared to be receiving visual information, and improved still further when given additional incentives. Thus his compartmentalization was relatively fluid and able to be modified by top-down intervention.
MECHANISMS OF COMPARTMENTALIZATION
Brown’s approach to this dissociative mechanism is in line with the model of dissociation as a dis-integration of frontal lobe processes. When our brains are processing experience in an integrated way, the areas of the frontal cortex that mediate consciousness, identity, memory, sensory awareness and emotion are working together – ie, the neural networks of each area are interconnected to form an integrative unit. When this integration is disrupted, the separate functions listed above can cause sensation, memory, cognition and/or emotion to be encoded separately, leading to a ‘compartmentalization’ of experience.
In other words, an individual may emerge from a traumatic experience (or series of traumatic experiences) with one or more parts of it ‘missing’. Some information from the experience may be unable to be retrieved through normal mental processing. This is not always experienced as amnesia, depending on which part of the experience was compartmentalized.
For me personally, the really fascinating part of Brown’s article is his hypothesis of how the compartmentalization process might actually happen in the brain. He describes this under the sub-heading ‘Consciousness and Cognitive Control’, page 13. His discussion is framed in dense and complex neurobiological language, which I have done my best to simplify and present in point form. My précis is under a separate tab for ease of access. It involves a L-O-N-G preamble explaining the brain’s cognitive architecture, how we process incoming information, and how that cognitive system might operate under normal and traumatic conditions. The final section offers a hypothesis on the formation of dissociated identities in DID.
LINK TO EXTRACT: Cognitive Processing and DID
Brown’s table below shows the traditional dissociative continuum. In the light of the ‘Two types of dissociation’ theory, the detachment type can be seen on the lower end of the continuum, with the compartmentalization type showing as a more severe, or fragmentary form of dissociation. This judgement about what is more or less severe might be questioned by someone whose life has been deeply affected by chronic depersonalization, for example. It is important to approach each person’s experience as unique and respect that their debilitation may not be commensurate with where they fall on this scale.
The exact neural pathways and mechanism of dissociation are not known definitively, but the moments of dissociation have been captured on MRI scans of large numbers of patients with dissociative identity disorder, at Swinburne University in Melbourne. The moments of switching from one state to another appear on the screen as massive disruptions of the subject’s brain waves, followed by a return to calm as the new state of consciousness (known as ‘alters’) settles in. (Ciorciari, 2012)
EARLIER MODEL OF DISSOCATION as proposed by Dan Siegel
Before the discovery that there seem to be two distinct forms of dissociation, psychiatry and psychology viewed the phenomenon as one single process which manifested in different ways, giving rise to disorders that needed different labels according to their symptom profile. However, Daniel J. Siegel recognised that this apparently single phenomenon was being driven or generated from two quite different systems, and it is significant that these two systems, the Parasympathetic Nervous System (part of the Autonomic Nervous System, or ANS) and the Information Processing System, are also the two key systems involved in the trauma response. Below are his descriptions of the two systemic expressions of dissociation. It can be clearly seen that the first, the ANS-driven dissociation has links to the later formulation of ‘detachment dissociation’, and the second, the Information Processing System of the neocortex, is moving towards a description of ‘compartmentalization’.
Dissociative Response driven by PARASYMPATHETIC NERVOUS SYSTEM
Allan Schore, in Healing Trauma (Solomon & Siegel, 2003), describes childhood attachment trauma and infant dissociation :
‘the child disengages from stimuli in the external world and attends to an ‘internal’ world. . . . When infants cannot repair failed interactions (with caregivers), they often lose postural control, withdraw, and self-comfort.
This behaviour is also associated with fixed, frozen, absent facial expression, absence of speaking, avoidance of eye contact, absence of relationship to others, and an impression that the person is out of reach.
It is thought that this defensive disengagement is mediated by the parasympathetic system of withdrawal/conservation (shut-down of the sympathetic system’s high-activity, emergency fight or flight response). When the person perceives themselves to be helpless in a hopelessly stressful situation, the primitive response is to freeze and attempt to become ‘unseen’ and avoid attention. This defense also conserves energy, allows ‘wounds’ to heal and hopefully recharges depleted inner resources.
The neurobiology of dissociation is therefore the opposite of the hyperarousal of the emergency stress response system, in which sugar-rich cortisols prime the body’s physical and psychological defense systems for action. Now the brain produces pain-numbing opioids (the naturally occurring ‘morphine’ in our brain) and action- inhibiting cortisols. In an instant, the individual can change from high alert to disengaged shut-down.
But neuroscientists also describe dissociation in terms of its relationship with the cardiovascular system and the ‘freeze response’. Since dissociation usually arises in relation to traumatic experience, the body is first subjected to high heart rate due to hyperarousal of the nervous system, and then to parasympathetic shut-down involving slowing down of heart rate and blood pressure. Research shows that the quick succession of these two states puts even more pressure on the cardiac system. The scientists describe it as ‘riding the gas and brake at the same time’, and brings on the freeze response.
Dissociation as disruption of the INFORMATION PROCESSING SYSTEM of the neocortex.
The functioning of the neocortex involves complex networks between its various regions, joined together by connections at the synapses. These interconnections link the memory function with our sense of self identity, awareness of consciousness and sensory perception of a world around us. If these functions are not linked into one integrated whole, we cannot operate in what is called a ‘normal’ way. For example, our sense of personal identity is closely linked to our memories, our awareness of consciousness is linked to sensory perception, which is also linked to our sense of identity (ie, my body ‘feels’ and looks as it does, so that is Me).
Dissociation is known to have an effect on the functioning of the cerebral cortex. The various processes described above are disrupted, possibly in the orbitofrontal region which co-ordinate these functions. The exact mechanism is not yet understood, but research has shown that a drug called Ketamine can block the transmission of signals across the synapses, especially those in the regions that associate identity, memory, consciousness and sensory perception. It is hypothesized that the separate regions for these functions become isolated from each other under the influence of dissociation.
In this way, a person can dissociate in and out of distinct and separate ‘selves’, if the memory and identity are uncoupled. The experience of a particular memory can ‘feel’ as if it belongs to a different part of oneself. Dissociation can result in experiencing a memory of the past or an event in the present as if it is happening to a part of you that you know is you but doesn’t feel like you.
Another common experience of dissociation, described by adults who were abused as children, involves sensory aberrations – experiencing the body as changing its shape, swelling up or becoming smaller, or visual alterations where bright coloured slivers fill the eyes’ vision, or directional sensing, where right and left become separate identities with separate realities. Many survivors of abuse describe their consciousness seeming to leave the body and float up above it. These are only a few of the many reported examples of sensory hallucination or cognitive alteration while dissociating.
Associational networks mediated by the Orbitofrontal Cortex (lower half of the Frontal Lobe, called ‘orbitofrontal’ as it lies behind the eyes)):
Emotional states Consciousness
Bodily responses Identity
Reasoning Memory
Memory retrieval Perception
Perceptual biases Social cognition
Appraisal of stimuli Regulation of emotion
The blockage of integrative circuits may separate these mental processes from one another and give rise to states of incoherence, disorientation, amnesia and other dissociative processes.
Imagine four of the main integrative circuits – Consciousness, Sensory Perception, Memory and Identity. The first graphic representation (1) imagines intact connections between these areas. Following (2,3,4 & 5) are some theoretical combinations of disconnection. It is interesting to stop and think about how one’s experience of reality would be affected, depending on which of these systems were involved in one’s compartmentalisation of experience :





Risk factors for dissociation :
younger age of victim,
higher levels of stress exposure,
greater subjective experiences of threat,
poorer general psychological health and adjustment,
weaker or more vulnerable identity formation (sense of self),
greater sense of external locus of control (ie, belief that you have no power in the situation),
more use of escape-avoidance and emotion-focused coping strategies,
rather than solution-focussed coping.
DISSOCIATION AND MEMORY
Once again, in educating oneself about the mechanisms of traumatisation, the link between memory and dissociation needs to be understood, so that informed choices can be made in the service of healing and recovery. In the moments of a potentially traumatizing event, focal attention is disrupted as the shocked and disoriented participant or observer automatically attempts to ‘escape’. The dissociative response kicks in, and this leads directly to an alteration in memory encoding, as described under ‘The Role of Memory in Trauma’.
MEMORY ENCODING
Memory is encoded in the left hemisphere (and note that in moments of fear, shock and panic, it is the right hemisphere that is more fully engaged. The left goes off-line to some extent.)
| Explicit memory (semantic/episodic) | Implicit memory |
| Requires focused attention | In the context of trauma:Divided attention (eg.dissociation) |
| Experienced as:I am recalling something | Experienced as:I am experiencing something -no sense of recalling past experience |
| Hippocampus encodes context-dependent information into the explicit memory network. This is why emotional or environmental cues can trigger memory.Context-dependent : emotional, sensory and environmental elements that were present at the event. |
The implicit memory system is not in the frontal cortex, is separate from the explicit system and mediated by the more primitive parts of the brain. This is why people with amnesia can still remember how to do things, learn new skills and have emotional associations. |
Divided attention experiment:
Earphones on left and right ears. List of zoo animals read into left ear, list of flowers read into right. Participants instructed to give focal attention to left ear, zoo animals.
Most will have good memory of zoo animals, most will have little memory of flowers.
BUT, when asked to fill in the spaces in a partially spelled word, ie, R – – E, they are more likely to put in ROSE (although other choices could be RISE, RIDE, RUDE, ROBE, ROLE, ROPE, etc.). The subjects have encoded the list of flowers implicity, and the brain is ‘primed’ to bring up a flower when cued. Subjects have no sense that they are recalling the word, or that what they are writing is something they experienced.
Without focal attention, items are not encoded explicity.
MEMORY RETRIEVAL
Memory is retrieved from the right hemisphere.
Cues can activate both explicit and implicit memory simultaneously. Recollections will often involve explicit elements associated with their implicit context-dependent counterparts.
SO, a client is telling you about her relationship with her alcoholic father. Suddenly she is overwhelmed with feeling, tears and shaking. She may compose herself and continue. What has happened is that she has been flooded with implicit elements of her childhood story. In composing herself, she pushed these implicit elements back down, to some extent dissociating from them, but will probably feel shaken for some time after.
This right hemisphere-retrieval connection is very significant when it comes to healing from trauma. The right hemisphere is also the location for the creative processes, so creative exercises (of many kinds) also create links and associations to implicit memory and seem to make it much easier to bring these implicit, traumatic memories up to consciousness. This is discussed more fully under ‘Healing – Arts Therapies’.
 Drawing out the image of the hurricane helped this child to be able to process the terrifying, traumatic memory of the event.
Drawing out the image of the hurricane helped this child to be able to process the terrifying, traumatic memory of the event.
[With permission: Art through the Eyes of Children
Art by displaced children at Renaissance Centre
http://www.katrinaexhibit.org]
More on Trauma
The Neurobiology of Psychological Trauma
An Evolutionary Model of Response to Danger
The Brain’s “Information Processing System”
Further Resources and Reading (Trauma)
